2. The normal concentrations of ammonia and other nitrogenous compounds in blood and other body fluids - Concentrations of citulline, arginine, and orotic acid
Please refer to figures 7 and 8
After glutamate, citrulline is next in importance for diagnosis of hyperammonaemia. It is decreased in proximal UCDs (intra-mitochondrial deficiencies of NAGS, CPS1 and OTC). Because citrulline levels can also be reduced in other conditions including deficiency of ATP synthase, P5C synthetase and some defects of the respiratory chain (e.g. NARP syndrome) as well as short bowel syndrome, the results should always be considered as part of the complete profile. However, citrulline is a specific marker of ASS and ASL deficiencies.
Arginine, being the metabolite immediately proximal to urea, reflects the overall activity of the urea cycle and, with the exception of arginase deficiency, might well be low in UCDs adding extra information for diagnosis.
Neither arginine nor citrulline levels in urine or CSF add any further information.
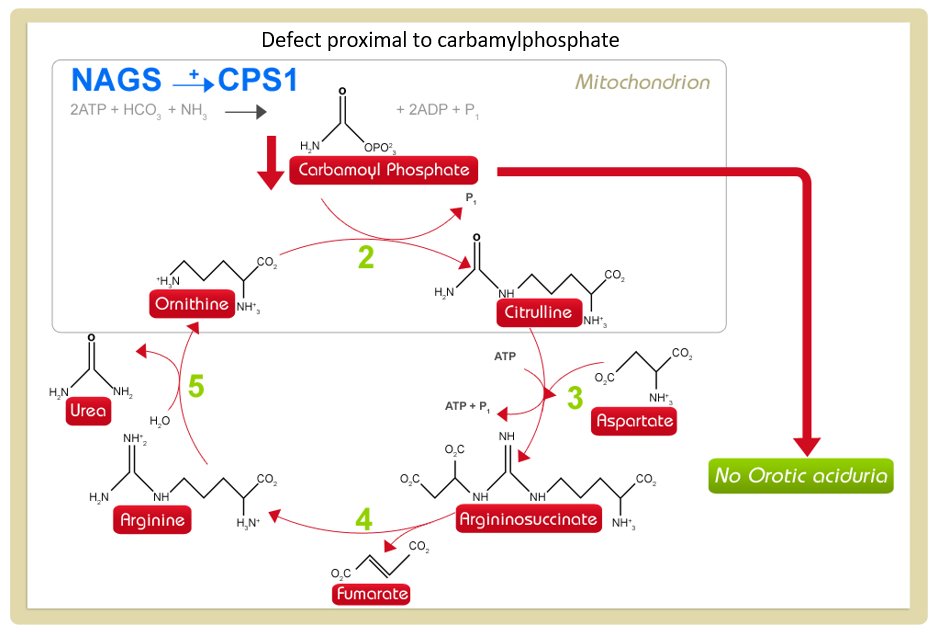
Orotic acid is part of the pyrimidine synthesis pathway and is normally present in only low concentrations in urine (2-5 mmol/mol creatinine). Whenever there is an accumulation of carbamoylphosphate, it spills over from the mitochondrion into the cytosol entering the pyrimidine synthesis pathway.
Urine orotic acid must be measured in all cases of hyperammonaemia to distinguish between OTC and NAGS or CPS1 deficiencies. Unfortunately, only liver enzyme analysis or gene mutation analysis will distinguish between NAGS and CPS1 deficiencies.
Most labs also measure the level of urine orotidine which is the metabolite directly distal to orotic acid and is often also elevated.
Figure 7: defect distal to carbamoylphosphate
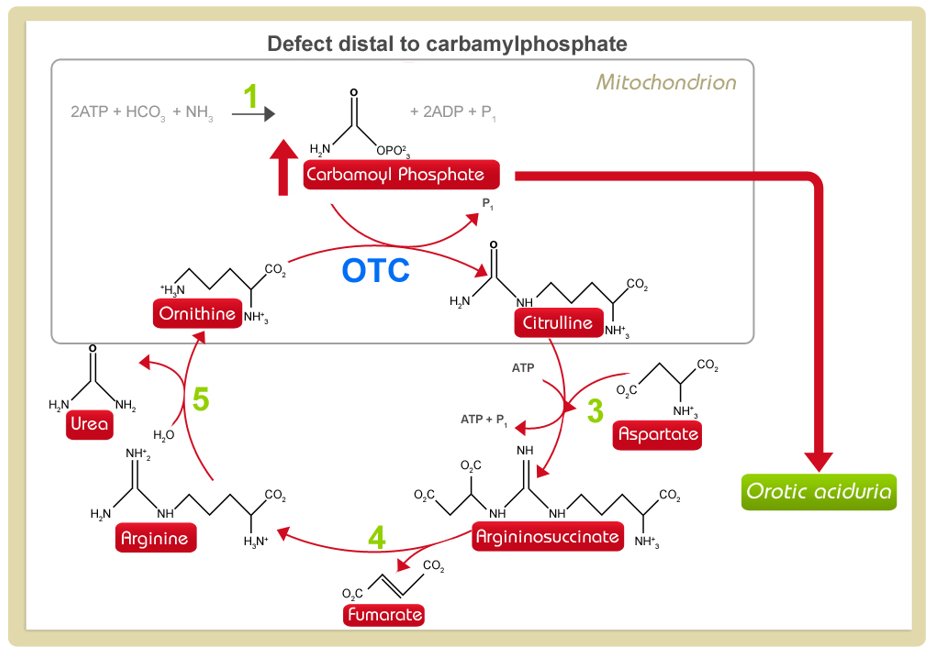
Figure 8: defect proximal to carbamoylphosphate